Why Not Augment the Breasts with Fat? Free Fat Grafting to the Breasts – A Warning
Breast augmentation is a simple, straightforward, effective procedure where an implant is placed behind the breast tissue to augment its volume. Sometimes an implant is required to correct the shape of the breasts, for instance in tubular breast augmentation.
Breast augmentation using implants provides natural results. The breast implant does not obscure future mammogram imaging or breast cancer detection, and most women are extremely happy with their results! It’s a great procedure! See before and after images of breast augmentation here.
But most importantly, breast augmentation using implants is REVERSIBLE. That’s correct – if a woman no longer wants her implants, they can simply be removed (often under local anesthesia as a short office procedure) – and the breasts will return to their pre-augmentation state.
This is something I offer to patients and perform routinely for women who do not want or need their implants anymore, for instance after weight gain or menopause-related increase in breast size.
There are very few possible long-term irreversible consequences of a breast augmentation. The breasts usually bounce back to their pre-augmentation state once the implant is removed.

Before breast augmentation – note post-partum breast deflation and loss of volume

After breast augmentation using smooth round silicone gel implants – results are natural and proportional!
I occasionally am asked the question by patients seeing me for a breast augmentation, “Can’t you inject my breasts with my own fat instead? Isn’t this more natural and better for me?”
Although there are options other than an implant that potentially can add volume to the breasts, such as:
- Injection of saline into the breasts for a “24-hour augmentation trial” (for $3000!) REALLY!?
- Free fat grafting or “lipo filling” the breasts using the body’s own fat
- Injection of illegal industrial substances are NOT approved by the FDA and not recommended by Board Certified Plastic Surgeons!
For several good reasons, I do not recommend free fat grafting to the breasts unless a woman is undergoing breast reconstruction – i.e. she has had a mastectomy for breast cancer or risk-reduction surgery (BRCA+ women), or for specific congenital conditions affecting the chest wall such as Poland’s Syndrome.

WHY NOT inject fat into the breasts?
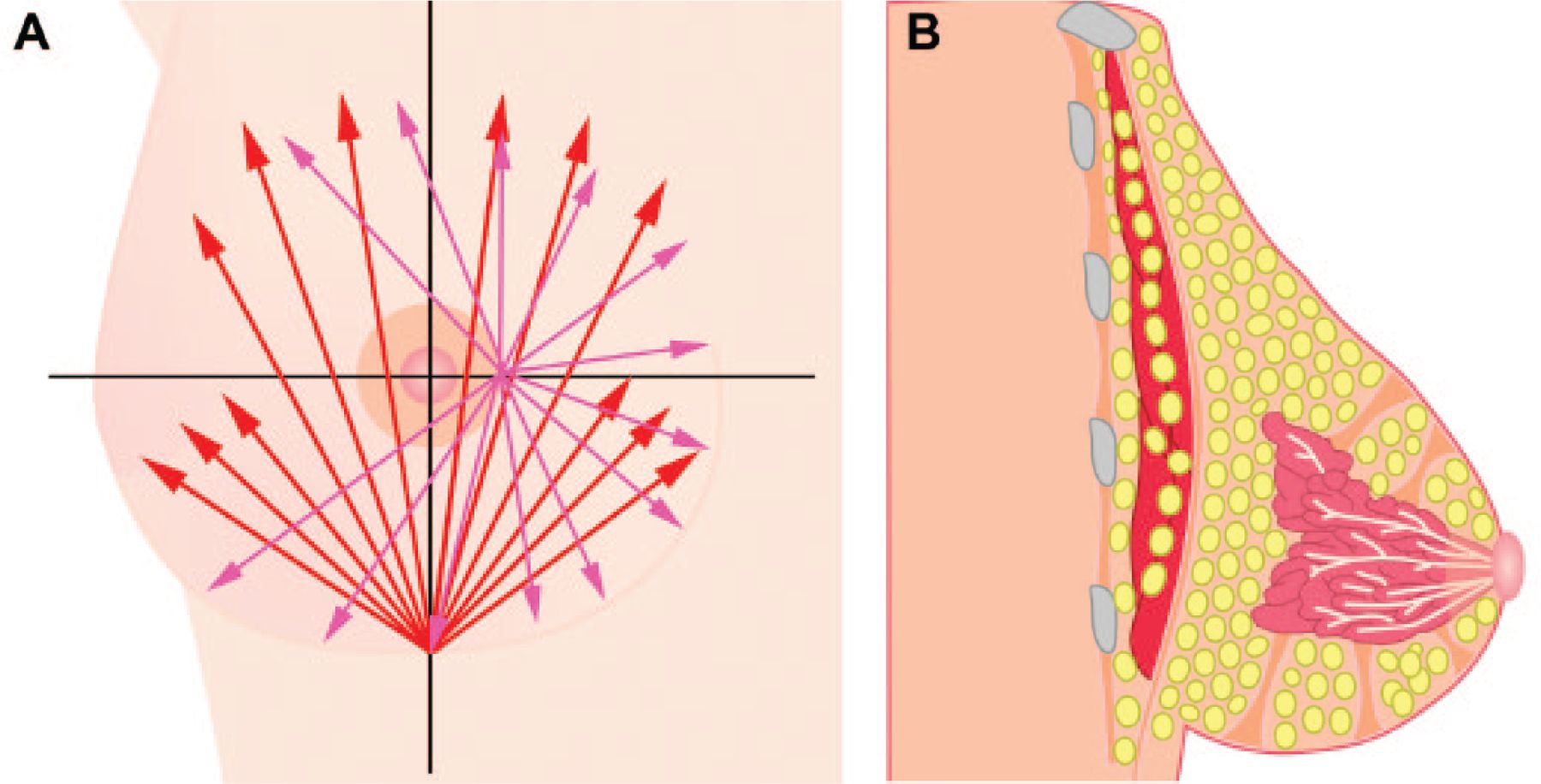
The reason for this recommendation is the following: when fat cells are removed using liposuction from one part of the body (usually the abdominal area, the hips or thighs), known as a “donor site”, the cells lose their native blood supply and are a free-floating. Hence, the term “free fat graft”. Free fat cells are then injected into another part of the body, such as the breasts, the buttocks, the lips, face or surface of the hands to add volume to these areas, in the hope that they will survive.
My website has an entire section which explains in detail the process of free fat grafting as an adjunct to breast reconstruction, which is also known as “lipo-filling”.
When fat cells are injected into a new location, known as the “recipient site”, some fat cells will persist in their new location and live, while others will not make it. We can only expect on average 30% of grafted fat cells to survive and to pick up an adequate blood supply. This is known as fat graft “take”.
The process of the body clearing fat cells which have not survived takes around 3 months. While the results of free fat grafting might look impressive immediately after surgery, within days swelling begins to go down and the fat which is not going to survive starts to melt away. Up to 70% of fat cells which don’t pick up a new blood supply will die and the body will naturally clear them.
This is not a dangerous process, just part of what happens with free fat grafting. However, when the event of clearing fat cells that have not “taken” or survived occurs, the dead fat cells can create calcifications or oil cysts. If grafted to the breasts, the fat cells that did not “take”, potentially obscuring mammogram findings and making breast cancer detection confusing or even dangerous!
The consequence of the fat cells that do not make it and which create calcifications or oil cysts are PERMANENT. Why on earth would any woman risk obscuring breast cancer detection for the rest of her life for a 30% increase in breast volume? And if multiple sessions of fat grafting are performed (which is usually recommended), the changes in the breast can be exponential and more extensive with multiple fat grafting procedures.
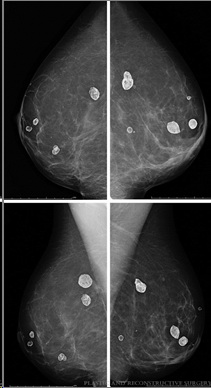
Oil cysts on a mammogram after free fat grafting – these could potentially obscure breast cancer screening
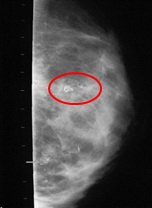
Calcifications on a mammogram after free fat grafting a normal breast – these may be indistinguishable from breast cancer calcifications
Unfortunately, I have been at professional society meetings where mammograms have been presented that are FULL of calcifications and oil cysts that look like a snowstorm! It is obvious that breast cancer screening is more difficult and that a woman would be at an increased risk of unnecessary biopsies and/or a breast cancer being missed because of the assumption that the mammogram abnormality might be due to previous fat grafting. YIKES!
Although some Radiologists claim they can effectively tell the difference between malignant calcifications and those resulting from the after-effects of fat grafting, why would anyone want to create this situation?
I perform a great deal of breast cancer reconstruction in my practice. I obviously feel strongly about this situation. I would NEVER put a woman at risk of obscuring breast cancer detection, mammogram abnormalities, false positive biopsies, fear of cancer while awaiting results after needing a biopsy, and/or the false sense of security that their abnormal mammogram was due to fat grafting and not a real finding of concern. It just isn’t worth it!

Unfortunately, some practitioners, many of which are not Board Certified Plastic Surgeons, or who are not surgeons at all, are NOT considering the long-term effects of what they are doing to the breasts, are actively marketing fat grafting to the breasts as “natural breast augmentation”. I shudder to think of what future mammograms will look like, particularly in young women who undergo this procedure and will not realize the effect of their procedure for 5, 10, 20 years when they have their first breast cancer screening.
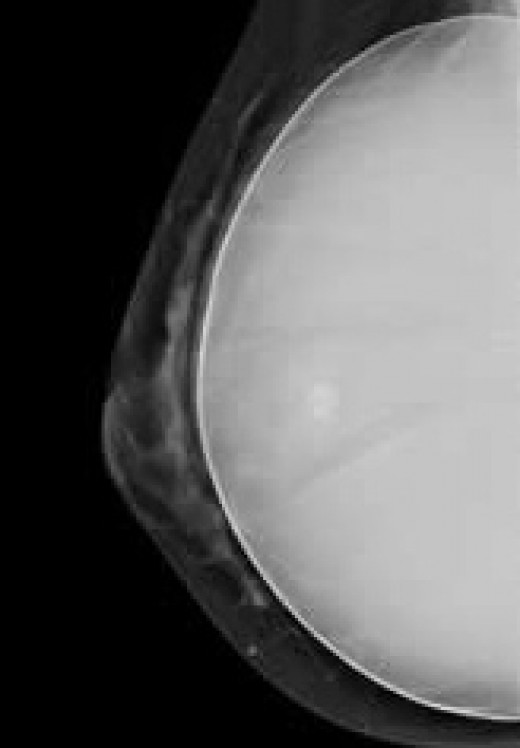
A breast implant is clearly visible on a mammogram and does not create the changes in the breast seen with fat grafting.
Placing a breast implant to augment a breast’s volume is SAFE, simple, and REVERSIBLE. A mammogram can clearly tell the difference between the breast tissue and the implant, and additional views are routinely used to ensure the entire surface of the breast is being visualized when an implant is in place. Placement of a breast implant on top or under the muscle does NOT affect mammogram imaging efficiency.
Breast augmentation using an implant does NOT create mammogram abnormalities such as calcifications, oil cysts or related imaging artifacts that can occur with free fat grafting to the breasts. So, these reasons are why I recommend AGAINST fat grafting to a natural breast! SAFETY is my #1 concern for all my patients, and is the the number one reason why I recommend for or against any procedure, and it is not worth the potential consequences to recommend fat grafting to a natural breast.
However, I do fat graft the chest wall for breast cancer reconstruction! After a mastectomy for breast cancer or as a risk-reduction surgery in BRCA+ women, no additional mammograms are performed because all breast tissue has been removed. Monitoring for breast cancer after mastectomy usually involves a physical examination by the Oncologist or Breast Surgeon, a PET scan or MRI or blood tests. Even if some calcifications or oil cysts occur, we will not be doing any future mammograms and their presence will be from the fat grafting, without consequence.

Fat grafting to the chest wall is now a commonplace procedure performed by Plastic Surgeons as a second-stage procedure after an implant or flap breast reconstruction
Free fat grafting is commonly used to help fill in a contour depression or a hollow resulting from the mastectomy removing much of the subcutaneous fat layer during the mastectomy. Fat grafting can slightly improve the contour of the chest wall in this situation, but it cannot be reliably used to build an entire breast.
Fat grafting can also be used to help fill in a chest wall depression resulting from a congenital condition where the pectoralis major muscle on one side is absent together with lack of development of the breast, known as Poland’s Syndrome. In this situation, the fat graft can be used to help fill in the depression resulting from an absent muscle immediately beneath the collar bone in the upper chest wall.
Note that in breast reconstruction, the fat graft is being injected into the chest wall, not the breast! Learn more about free fat grafting as an adjunct to breast reconstruction here.

I recommend that my patients discuss any concerns they might have about free fat grafting with their oncology team, who will discuss with them in detail the methods that will be used for monitoring after their breast cancer treatment and who usually give their blessing for fat grafting as an adjunct to breast implant reconstruction or free flap breast reconstruction such as the DIEP flap, SIEA flap or inner thigh (TUG) flap.
For more information about free fat grafting, visit this section of our website. To learn more about breast augmentation, read our educational blog posts. View before and after photos in our breast augmentation gallery.
To schedule a consultation with Dr. Horton, complete our online consultation request form or call 415-923-3067 today!